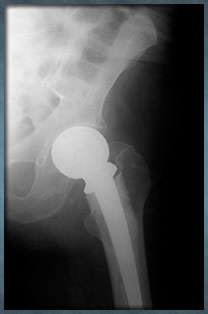
If you or a loved received a metal on metal hip implant, contact the Steinberg Law Firm.
888-529-4688
andrewsteinberg@lawyer.com
Houston 3200 Travis : 3rd Floor Houston, TX 77006 (713) 529-0025 (713) 751-0412 (fax)
Galveston (409) 762-9090
Toll Free 888-529-4688
andrewsteinberg@lawyer.com www.thesteinberglawfirm.com
Free Case Review
Fill out the form below if you need additional information or want to discuss a potential claim with an attorney. All inquiries are kept strictly confidential.
* denotes required field
How would you prefer to be contacted?